
Abstract
Fibromyalgia (FM) is a chronic pain disorder that affects approximately 2%-3% of US adults, occurs predominantly in women, and is characterized by widespread pain, nonrestorative sleep, fatigue, cognitive dysfunction, and functional impairment. Tonmya® (TNX-102 SL; cyclobenzaprine HCl sublingual tablets [CBP SL]) is FDA-approved for the treatment of FM in adults based on the results from two Phase 3 trials (RESILIENT and RELIEF).
Here, the efficacy of CBP SL in the treatment of pain associated with FM is assessed via responder analyses from the RESILIENT and RELIEF trials; safety findings are also reported.
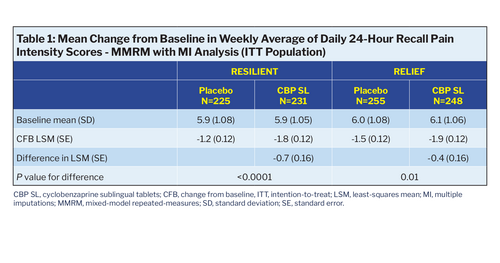
The primary endpoint in both studies was the change from baseline in weekly average of daily pain numeric rating scale scores at Week 14, analyzed using mixed model repeated measures with multiple imputation for missing data. In both studies, CBP SL treatment resulted in significant improvements in the primary endpoint (RESILIENT, P<0.0001 and RELIEF, P=0.010). A responder analysis was performed to evaluate clinically meaningful reduction in pain, defined as a ≥30% reduction in the primary endpoint. A ≥50% responder analysis was also conducted. Safety assessments included reporting of adverse events (AEs).
In RESILIENT, CBP SL produced higher response rates than placebo for both the ≥30% responder threshold (45.9% vs 27.1%; P<0.001, uncorrected) and the ≥50% threshold (22.5% vs 13.3%; P=0.011, uncorrected). In RELIEF, corresponding uncorrected P-values were P=0.006 for ≥30%, and P=0.141 for ≥50% pain response. CBP SL was generally well tolerated,
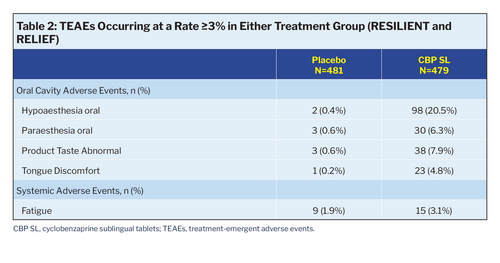
with a safety profile consistent with prior studies and no new safety signals. The most common AE was transient tongue numbness, which was mild, self-limited, and uncommonly led to study discontinuation.
CBP SL demonstrated significant pain reductions and clinically meaningful improvements in the RESILIENT and RELIEF trials, making it a promising treatment option and the first FDA- approved treatment for adults with FM in over 15 years.
Here, the efficacy of CBP SL in the treatment of pain associated with FM is assessed via responder analyses from the RESILIENT and RELIEF trials; safety findings are also reported.
The primary endpoint in both studies was the change from baseline in weekly average of daily pain numeric rating scale scores at Week 14, analyzed using mixed model repeated measures with multiple imputation for missing data. In both studies, CBP SL treatment resulted in significant improvements in the primary endpoint (RESILIENT, P<0.0001 and RELIEF, P=0.010). A responder analysis was performed to evaluate clinically meaningful reduction in pain, defined as a ≥30% reduction in the primary endpoint. A ≥50% responder analysis was also conducted. Safety assessments included reporting of adverse events (AEs).
In RESILIENT, CBP SL produced higher response rates than placebo for both the ≥30% responder threshold (45.9% vs 27.1%; P<0.001, uncorrected) and the ≥50% threshold (22.5% vs 13.3%; P=0.011, uncorrected). In RELIEF, corresponding uncorrected P-values were P=0.006 for ≥30%, and P=0.141 for ≥50% pain response. CBP SL was generally well tolerated,
with a safety profile consistent with prior studies and no new safety signals. The most common AE was transient tongue numbness, which was mild, self-limited, and uncommonly led to study discontinuation.
CBP SL demonstrated significant pain reductions and clinically meaningful improvements in the RESILIENT and RELIEF trials, making it a promising treatment option and the first FDA- approved treatment for adults with FM in over 15 years.
Introduction
Fibromyalgia (FM) is a chronic pain disorder that affects approximately 2%-3% of US adults, occurs predominantly in women, and is characterized by widespread pain, nonrestorative sleep, fatigue, cognitive dysfunction, and functional impairment. More recently, FM has been understood as the prototypic “nociplastic syndrome” as discussed by Clauw [1]. Nociplastic pain, a third category of pain distinct from nociceptive pain and neuropathic pain, is characterized by pain arising from altered nociception despite a lack of pathology in peripheral nociceptors. Nociplastic pain is driven by dysregulation in the processing of pain signals within the central nervous system (CNS) and may involve changes in neurotransmitter levels, central sensitization, insufficient deep sleep, and maladaptive neuroplasticity, all of which can amplify pain perception
and contribute to the persistent, diffuse pain that typifies FM.
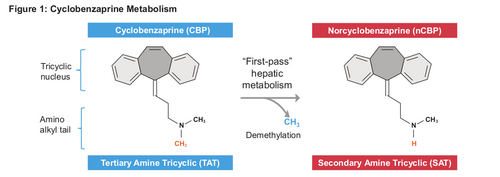
Approximately 50 years ago, Dr. Harvey Moldofsky recognized the role of nonrestorative sleep in the pathogenesis and persistence of FM [2,3]. Individuals with FM typically suffer from disruptions in the deep restorative stages of sleep, and poor sleep quality is highly associated with the exacerbation and perpetuation of nociplastic pain. Traditional analgesics like NSAIDs or opioids in nociplastic syndrome often prove ineffective if not deleterious; furthermore, patient dissatisfaction is common with currently approved products for FM. Cyclobenzaprine HCl (CBP) is a tertiary amine tricyclic (TAT) metabolized in the liver via demethylation to norcyclobenzaprine (nCBP), an active secondary amine tricyclic metabolite (Figure 1). With daily oral immediate- release (IR) cyclobenzaprine administration, the pharmacokinetic (PK) profile for CBP is dynamic, with a relatively short half-life. In contrast, nCBP has a significantly longer half-life, leading to its accumulation, a flattened PK profile, and steady-state concentrations that exceed those of CBP. nCBP not only interferes with the receptor binding of CBP but also is a uniquely potent inhibitor of the norepinephrine transporter, which may disrupt restorative sleep, acting against the proposed mechanism of the parent molecule. Like other TATs, oral IR CBP was poorly tolerated (ie, increased frequency of systemic adverse events) in clinical studies, potentially due to reduced receptor binding caused by nCBP accumulation over weeks with daily dosing. Previous studies of oral IR CBP in treating FM demonstrated short-lived improvements in sleep without significant benefits to pain or fatigue, as discussed by Carette et al. [4].
Tonmya® (TNX-102 SL; cyclobenzaprine HCl sublingual tablets [CBP SL]) is an innovative sublingual tablet formulation of CBP, distinct from oral CBP in providing rapid sublingual transmucosal absorption, greater bioavailability, and reduced production of nCBP due to bypassing of first-pass hepatic metabolism as discussed by Daugherty et al. [5,6]. On the basis of the results from two Phase 3 trials (RESILIENT and RELIEF), CBP SL is the first FDA-approved treatment for adults with
FM in over 15 years [7,8]. Among its activities, CBP potently binds and antagonizes the 5-HT2A- serotonergic, α1-adrenergic, M1-muscarinic acetylcholine, and H1-histaminergic receptors, each of which impacts aspects of sleep architecture. CBP SL is hypothesized to work by targeting nonrestorative sleep, a core characteristic of FM.
Here, the efficacy of CBP SL in the treatment of pain associated with FM is assessed via responder analyses from the RESILIENT and RELIEF trials; safety findings are also reported.
and contribute to the persistent, diffuse pain that typifies FM.
Approximately 50 years ago, Dr. Harvey Moldofsky recognized the role of nonrestorative sleep in the pathogenesis and persistence of FM [2,3]. Individuals with FM typically suffer from disruptions in the deep restorative stages of sleep, and poor sleep quality is highly associated with the exacerbation and perpetuation of nociplastic pain. Traditional analgesics like NSAIDs or opioids in nociplastic syndrome often prove ineffective if not deleterious; furthermore, patient dissatisfaction is common with currently approved products for FM. Cyclobenzaprine HCl (CBP) is a tertiary amine tricyclic (TAT) metabolized in the liver via demethylation to norcyclobenzaprine (nCBP), an active secondary amine tricyclic metabolite (Figure 1). With daily oral immediate- release (IR) cyclobenzaprine administration, the pharmacokinetic (PK) profile for CBP is dynamic, with a relatively short half-life. In contrast, nCBP has a significantly longer half-life, leading to its accumulation, a flattened PK profile, and steady-state concentrations that exceed those of CBP. nCBP not only interferes with the receptor binding of CBP but also is a uniquely potent inhibitor of the norepinephrine transporter, which may disrupt restorative sleep, acting against the proposed mechanism of the parent molecule. Like other TATs, oral IR CBP was poorly tolerated (ie, increased frequency of systemic adverse events) in clinical studies, potentially due to reduced receptor binding caused by nCBP accumulation over weeks with daily dosing. Previous studies of oral IR CBP in treating FM demonstrated short-lived improvements in sleep without significant benefits to pain or fatigue, as discussed by Carette et al. [4].
Tonmya® (TNX-102 SL; cyclobenzaprine HCl sublingual tablets [CBP SL]) is an innovative sublingual tablet formulation of CBP, distinct from oral CBP in providing rapid sublingual transmucosal absorption, greater bioavailability, and reduced production of nCBP due to bypassing of first-pass hepatic metabolism as discussed by Daugherty et al. [5,6]. On the basis of the results from two Phase 3 trials (RESILIENT and RELIEF), CBP SL is the first FDA-approved treatment for adults with
FM in over 15 years [7,8]. Among its activities, CBP potently binds and antagonizes the 5-HT2A- serotonergic, α1-adrenergic, M1-muscarinic acetylcholine, and H1-histaminergic receptors, each of which impacts aspects of sleep architecture. CBP SL is hypothesized to work by targeting nonrestorative sleep, a core characteristic of FM.
Here, the efficacy of CBP SL in the treatment of pain associated with FM is assessed via responder analyses from the RESILIENT and RELIEF trials; safety findings are also reported.
Materials & Methods
Two pivotal 14-week, randomized, double-blind, placebo-controlled studies were conducted in subjects with FM: RESILIENT (NCT05273749) and RELIEF (NCT04172831), each reported by Lederman et al. [7,8]. Both studies randomized subjects 1:1 to receive CBP SL 2.8 mg for 2 weeks followed by 5.6 mg for 12 weeks or matching placebo for 14 weeks. The primary endpoint was the change from baseline to Week 14 in weekly average of daily self-reported average pain numeric rating scale scores analyzed by mixed-model repeated-measures analysis, with multiple imputation for missing data. Clinically meaningful improvements in pain were also analyzed via proportions of subjects with a ≥30% and ≥50% improvement from baseline to Week 14 in the weekly average of daily self-reported average pain severity scores. Safety was assessed by adverse events, vital signs/weight, physical exams, clinical lab tests, Columbia-Suicide Severity Rating Scale (C-SSRS), and Beck Depression Inventory II.
Results
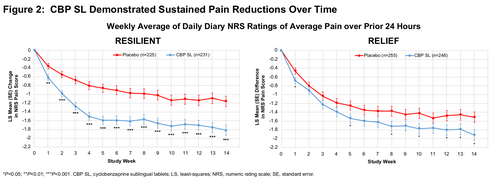
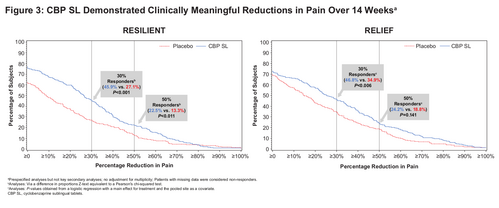
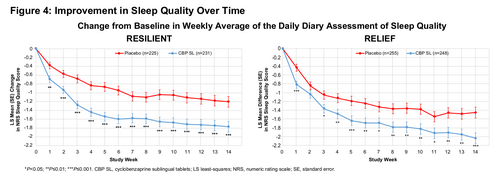
Baseline characteristics and demographics were well-balanced between CBP SL and placebo in both trials (Table 1). CBP SL treatment provided statistically significant improvements over placebo on the primary endpoint (pain reduction) at Week 14; primary endpoint results of both trials are presented by study week in Figure 2. In RESILIENT, compared with the placebo group, the CBP SL group had a higher proportion with ≥30% pain response (45.9% vs 27.1%; P<0.001, uncorrected) and ≥50% pain response (22.5% vs 13.3%; P=0.011, uncorrected). In RELIEF, CBP SL treatment resulted in higher proportion of patients with ≥30% pain response (46.8% vs 34.9%, respectively; P=0.006, uncorrected) and ≥50% pain response (24.2% vs 18.8%, respectively; P=0.141, uncorrected) compared with placebo (Figure 3). Significant improvements in the change from baseline in the weekly average of the daily diary assessment of sleep quality, a key secondary endpoint, was observed in both trials (Figure 4). CBP SL was generally well tolerated, with a low incidence of systemic TEAEs; fatigue was the only systemic TEAE that occurred at a rate ≥3%. The most common TEAEs were oral administration site reactions, tongue/mouth numbness or tingling and bitter aftertaste, which were typically transient, self-limited, not severe, and uncommonly led to discontinuation (Table 2).
Conclusions
FM is the prototypic nociplastic syndrome and chronic overlapping pain condition with CNS symptoms of widespread pain, nonrestorative sleep, fatigue, and cognitive dysfunction. By pharmacologically targeting nonrestorative sleep, treatment with daily bedtime CBP SL resulted in substantial and clinically meaningful pain relief. CBP SL was generally well tolerated, with an AE profile consistent with previous studies; no new safety signals were observed. Together, these findings are consistent with the concept that disturbed sleep in FM is an obstacle to recovery and pharmacological targeting of nonrestorative sleep may facilitate recovery.
Figures
TABLES
References
1. Clauw DJ. Ann Rheum Dis. 2024;83(11):1421-7.
2. Moldofsky H, et al. Psychosom Med. 1975;37(4):341-51.
3. Moldofsky H, Scarisbrik P. Psychosom Med. 1976;38(1):35-44.
4. Carette S, et al. Arthritis Rheum. 1994;37(1):32-40.
5. TONMYA™ (cyclobenzaprine hydrochloride sublingual tablets) [prescribing information]. Chatham, NJ: Tonix Medicines, Inc; 2025.
6. Daugherty BL, et al. Clin Pharmacol Drug Dev. 2026;15(3):e70034.
7. Lederman S, et al. Pain Med. 2026;27(1)86-94.
8. Lederman S, et al. Arthritis Care Res (Hoboken). 2023;75(11):2359-68.
2. Moldofsky H, et al. Psychosom Med. 1975;37(4):341-51.
3. Moldofsky H, Scarisbrik P. Psychosom Med. 1976;38(1):35-44.
4. Carette S, et al. Arthritis Rheum. 1994;37(1):32-40.
5. TONMYA™ (cyclobenzaprine hydrochloride sublingual tablets) [prescribing information]. Chatham, NJ: Tonix Medicines, Inc; 2025.
6. Daugherty BL, et al. Clin Pharmacol Drug Dev. 2026;15(3):e70034.
7. Lederman S, et al. Pain Med. 2026;27(1)86-94.
8. Lederman S, et al. Arthritis Care Res (Hoboken). 2023;75(11):2359-68.
Conflicts of Interest
EG: Employee of Tonix Medicines, Inc. and stock ownership in Tonix Pharmaceuticals Holding Corp.
MK, JH, GMS: Employee of Tonix Pharmaceuticals, Inc. and stock ownership in Tonix Pharmaceuticals Holding Corp.
MK, JH, GMS: Employee of Tonix Pharmaceuticals, Inc. and stock ownership in Tonix Pharmaceuticals Holding Corp.
Funding Statement
Tonix Pharmaceuticals, Inc.