
Audio Presentation
Abstract
Background
Acute pancreatitis is characterized by severe visceral pain that remains challenging to manage despite multimodal analgesic approaches including opioids therapy (1-4). In refractory cases, alternative analgesic approaches targeting central sensitization may be required (5-7). Ketamine, a non-competitive N-methyl-D-aspartate (NMDA) receptor antagonist, has emerged as a potential option for severe acute pain (5,8-10).
Objective
To report the analgesic efficacy and safety of low-dose intravenous ketamine in two patients with severe acute pancreatitis pain refractory to standard analgesic therapy.
Methods
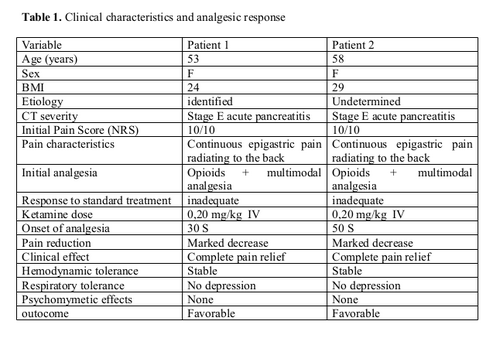
We describe two female patients admitted to the emergency department withsevere acute pancreatitis confirmed by abdominal computed tomography (stage E). Both patients presented with intense continuous epigastric pain (numerical rating scale [NRS] 10/10) refractory to conventional multimodal analgesia including opioids. Intravenous ketamine was administered at a subanesthetic dose of 0,20mg/kg under continuous monitoring.
Results
Both patients (between 50 and 60 yars old, BMI 24-29 kg/m2) experienced rapid and marked pain relief within minutes following ketamine administration, with a significant reduction in NRS scores and improved comfort. No hemodynamic instability, respiratory depression, or psychomimetic adverse affects were observed.
Conclusion
Low-dose ketamine may represent an effective and safe rescue analgesic option for refractory pain in severe acute pancreatitis. Larger prospective studies are needed to confirm its efficacy, safety, and optimal dosing strategies.
Acute pancreatitis is characterized by severe visceral pain that remains challenging to manage despite multimodal analgesic approaches including opioids therapy (1-4). In refractory cases, alternative analgesic approaches targeting central sensitization may be required (5-7). Ketamine, a non-competitive N-methyl-D-aspartate (NMDA) receptor antagonist, has emerged as a potential option for severe acute pain (5,8-10).
Objective
To report the analgesic efficacy and safety of low-dose intravenous ketamine in two patients with severe acute pancreatitis pain refractory to standard analgesic therapy.
Methods
We describe two female patients admitted to the emergency department withsevere acute pancreatitis confirmed by abdominal computed tomography (stage E). Both patients presented with intense continuous epigastric pain (numerical rating scale [NRS] 10/10) refractory to conventional multimodal analgesia including opioids. Intravenous ketamine was administered at a subanesthetic dose of 0,20mg/kg under continuous monitoring.
Results
Both patients (between 50 and 60 yars old, BMI 24-29 kg/m2) experienced rapid and marked pain relief within minutes following ketamine administration, with a significant reduction in NRS scores and improved comfort. No hemodynamic instability, respiratory depression, or psychomimetic adverse affects were observed.
Conclusion
Low-dose ketamine may represent an effective and safe rescue analgesic option for refractory pain in severe acute pancreatitis. Larger prospective studies are needed to confirm its efficacy, safety, and optimal dosing strategies.
Introduction
Acute pancreatitis is a common inflammatory condition associated with severe visceral pain, often described as a deep, continuous, and radiating to the back. Pain control remains a major clinical challenge despite the use of multimodal analgesia including non-opioid agents and apioids (1-4).
In some patients, standard treatment fails to provide adequate relief, leading to persistent suffering and increased opioid requirements. This phenomenon is partly explained by the complex pathophysiology of pancreatic pain, whitch involves peripheral nociceptor activation, neurogenic inflammation, and central sensitization (11-13).
A key mechanism in persistent pain states is the activation of N-methyl-D-aspartate (NMDA) receptors in the dorsal horn of the spinal cord, contributing to wind-up phenomena and amplification of nociceptive signaling (5,7,14).
Ketamine, a non-competitive NMDA receptor antagonist, has been increasingly used in subanesthesic doses in acute and chronic pain conditions. Its analgesic properties include inhibition of central sensitization and modulation of opioid- induced hyperalgesia. The aim of this report is to describe the clinical response to low dose ketamine in two cases of severe acute pancreatitis pain refractory to conventional therapy.
Pathophysiology (Figure 1)
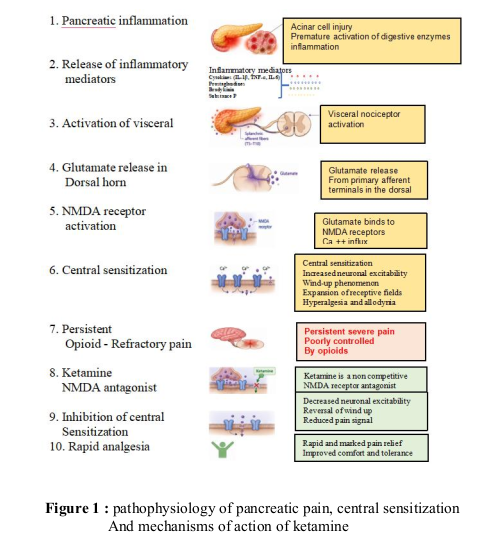
Pain in acute pancreatitis results from a combination of inflammatory and neurogenic machanisms (11-13). Intrapancreatic enzyme activation leads to tissue injury and release of pro-inflammatory mediators including cytokines, prostaglandins and bradykinin, whitch activate visceral nociceptors.
Pain signals are transmitted via splanchnic afferent fibers (T5-T10) through the celiac plexus to the dorsal horn of the spinal cord. Sustaines nociceptive input leads to glutamate release and activation of NMDS receptores, resulting in central sensitization and amplification of pain transmission (5,7,11,14).
This neuroplastic process contributes to hyperalgesia and reduced response to conventional analgesics, providing a rationale for NMDA receptor antagonism using ketamine (6,7,14,15).
In some patients, standard treatment fails to provide adequate relief, leading to persistent suffering and increased opioid requirements. This phenomenon is partly explained by the complex pathophysiology of pancreatic pain, whitch involves peripheral nociceptor activation, neurogenic inflammation, and central sensitization (11-13).
A key mechanism in persistent pain states is the activation of N-methyl-D-aspartate (NMDA) receptors in the dorsal horn of the spinal cord, contributing to wind-up phenomena and amplification of nociceptive signaling (5,7,14).
Ketamine, a non-competitive NMDA receptor antagonist, has been increasingly used in subanesthesic doses in acute and chronic pain conditions. Its analgesic properties include inhibition of central sensitization and modulation of opioid- induced hyperalgesia. The aim of this report is to describe the clinical response to low dose ketamine in two cases of severe acute pancreatitis pain refractory to conventional therapy.
Pathophysiology (Figure 1)
Pain in acute pancreatitis results from a combination of inflammatory and neurogenic machanisms (11-13). Intrapancreatic enzyme activation leads to tissue injury and release of pro-inflammatory mediators including cytokines, prostaglandins and bradykinin, whitch activate visceral nociceptors.
Pain signals are transmitted via splanchnic afferent fibers (T5-T10) through the celiac plexus to the dorsal horn of the spinal cord. Sustaines nociceptive input leads to glutamate release and activation of NMDS receptores, resulting in central sensitization and amplification of pain transmission (5,7,11,14).
This neuroplastic process contributes to hyperalgesia and reduced response to conventional analgesics, providing a rationale for NMDA receptor antagonism using ketamine (6,7,14,15).
Methods
We conducted a descriptive cases series of two patients admitted to the emergency department
for severe acute pancreatitis. The study was observational in design and aimed to describe the
clinical response to low-dose intravenous ketamine in patients with refractory pain. The following variables were collected : age, sex, and body mass index (BMI): pain intensity assessed using Numerical Rating Scale (NRS, 0-10); clinical presentation; etiology of pancreatitis; imaging findings, analgesic management; response to treatment, including onset, magnitude, and duration of analgesia; and overall clinical outcome. Both patients presented with severe, continuous epigastric pain radiating to the back, associated with an NRS score of 10/10. Clinical symptoms included nausea, abdominal
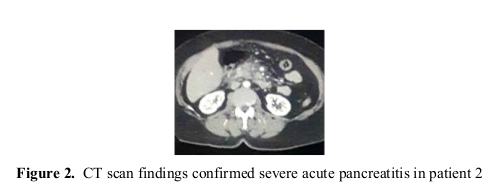
tenderness, and subfebrile temperature. The diagnosis of severe acute pancreatitis (stage E) was confirmed by contrast-enhanced computed tomography (Figure 2). Initial management consisted of standard multimodal analgesia, including opioid and non- opioid agents; however, pain control remained inadequate despite these interventions. Intravenous ketamine was subsequently administered at a dose of 0,20 mg/kg under continuous cardiorespiratory monitoring.
for severe acute pancreatitis. The study was observational in design and aimed to describe the
clinical response to low-dose intravenous ketamine in patients with refractory pain. The following variables were collected : age, sex, and body mass index (BMI): pain intensity assessed using Numerical Rating Scale (NRS, 0-10); clinical presentation; etiology of pancreatitis; imaging findings, analgesic management; response to treatment, including onset, magnitude, and duration of analgesia; and overall clinical outcome. Both patients presented with severe, continuous epigastric pain radiating to the back, associated with an NRS score of 10/10. Clinical symptoms included nausea, abdominal
tenderness, and subfebrile temperature. The diagnosis of severe acute pancreatitis (stage E) was confirmed by contrast-enhanced computed tomography (Figure 2). Initial management consisted of standard multimodal analgesia, including opioid and non- opioid agents; however, pain control remained inadequate despite these interventions. Intravenous ketamine was subsequently administered at a dose of 0,20 mg/kg under continuous cardiorespiratory monitoring.
FIGURES
Results
Both patients were female, aged 50-60 years old, a BMI of 24 to 29 kg/m2. Etiological cause was identified in one patient (Table 1).
Despite adequate opioid-based analgesia, pain remained severe (NRS 10/10).
Following ketamine administration after informed consent was obtained from the patients :
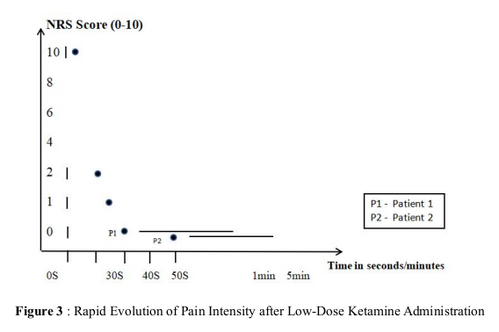
Onset of analgesia occured within 30-60 seconds (Figure 3)
NRS decreased markedly in less than one minute
Complete pain relief was achieved
Significant improvement in comfort and clinical tolerance was observed
No adverse effects were reported, including psychomimetic symptoms, respiratory depression
or hemodynamic instability. Clinical evolution was favorable in both cases.
Despite adequate opioid-based analgesia, pain remained severe (NRS 10/10).
Following ketamine administration after informed consent was obtained from the patients :
Onset of analgesia occured within 30-60 seconds (Figure 3)
NRS decreased markedly in less than one minute
Complete pain relief was achieved
Significant improvement in comfort and clinical tolerance was observed
No adverse effects were reported, including psychomimetic symptoms, respiratory depression
or hemodynamic instability. Clinical evolution was favorable in both cases.
Discussions
These case reports highlight the potential role of low-dose ketamine as a rescue analgesic in
severe acute pancreatitis refractory to conventional therapy. The rapid onset of analgesia can be explained by ketamine’s high lipid solubility and rapid
penetration of the blood-brain barrier, allowing immediate modulation of NMDA receptor- mediated nociceptive transmission (5,8,10). Previous studies in emergency department settings have reported that low-dose intravenous
ketamine provides analgesia within several minutes of administration, typically ranging from
5 to 15 minutes; however, in our cases, onset of analgesia occured within 30-60 seconds, suggesting an exceptionally rapid clinical response compared to published data (10,16, 17).
The sustained analgesic effect is likely related to interruption of central sensitization processes, reducing neuronal hyperexcitability within the spinal dorsal horn (5,7,14). Beyond NMDA antagonism, ketamine may also modulate descending inhibitory pathways and opioid receptor activity, contributing to its analgesic profile (8,10,14). Our observations are consistent with increasing evidence supporting the use of ketamine in acute pain emergencies, particularly in opioid-refractory conditions (5,8-10,16-20). In the literature, ketamine has been shown to reduce opioid requirements and improve
analgesia in acute pain settings, including emergency department protocols and perioperative
management, supporting its role as an opioid-sparing agent (17,20).
The absence of significant adverse effects in our cases supports the safety of carefully monitored subanesthesic dosing in emergency settings (5,8-10). However, this report is limited by its small sample size, observational design, and lack of long-term follow-up. Severe acute pancreatitis is recognized as one of the most intense forms of visceral pain, aften associated with marked activation of central sensitization pathways, which may explain the reduced response to conventional opioid-based analgesia (11-13).
Although evidence remains limited, case-bases literature suggests that ketamine may be beneficial in refractory abdominal and pancreatic pain, particulary when standard multimodal analgesia fails (11,17).
Current understanding of pain mechanisms in acute pancreatitis supports the involvement of NMDA receptor activation and glutaminergic transmission in dorsal horn sensitization, providing a strong pharmacological rationale for the use of ketamine in this context (5,7,11, 14).
However, the available clinical evidence remains limited to case reports and small observational studies, highlighting the need for prospective controlled trials to better define its efficacy and optimal dosing in acute pancreatitis pai management (5,8-10,16-20).
Limitations
This report has several limitations. First, the sample size was extremely small, with only two patients included, which limits the scope and generalizability of the findings. Second, the observational nature of the report, together with the absence of a control group does not allow definitive conclusions regarding the efficacy of low-dose ketamine to be established. In addition, analgesic outcomes were assessed only in the short term, without evaluation of prolonged effects or pain recurrence. Finally, follow-up duration was not standardized
between the two cases.
severe acute pancreatitis refractory to conventional therapy. The rapid onset of analgesia can be explained by ketamine’s high lipid solubility and rapid
penetration of the blood-brain barrier, allowing immediate modulation of NMDA receptor- mediated nociceptive transmission (5,8,10). Previous studies in emergency department settings have reported that low-dose intravenous
ketamine provides analgesia within several minutes of administration, typically ranging from
5 to 15 minutes; however, in our cases, onset of analgesia occured within 30-60 seconds, suggesting an exceptionally rapid clinical response compared to published data (10,16, 17).
The sustained analgesic effect is likely related to interruption of central sensitization processes, reducing neuronal hyperexcitability within the spinal dorsal horn (5,7,14). Beyond NMDA antagonism, ketamine may also modulate descending inhibitory pathways and opioid receptor activity, contributing to its analgesic profile (8,10,14). Our observations are consistent with increasing evidence supporting the use of ketamine in acute pain emergencies, particularly in opioid-refractory conditions (5,8-10,16-20). In the literature, ketamine has been shown to reduce opioid requirements and improve
analgesia in acute pain settings, including emergency department protocols and perioperative
management, supporting its role as an opioid-sparing agent (17,20).
The absence of significant adverse effects in our cases supports the safety of carefully monitored subanesthesic dosing in emergency settings (5,8-10). However, this report is limited by its small sample size, observational design, and lack of long-term follow-up. Severe acute pancreatitis is recognized as one of the most intense forms of visceral pain, aften associated with marked activation of central sensitization pathways, which may explain the reduced response to conventional opioid-based analgesia (11-13).
Although evidence remains limited, case-bases literature suggests that ketamine may be beneficial in refractory abdominal and pancreatic pain, particulary when standard multimodal analgesia fails (11,17).
Current understanding of pain mechanisms in acute pancreatitis supports the involvement of NMDA receptor activation and glutaminergic transmission in dorsal horn sensitization, providing a strong pharmacological rationale for the use of ketamine in this context (5,7,11, 14).
However, the available clinical evidence remains limited to case reports and small observational studies, highlighting the need for prospective controlled trials to better define its efficacy and optimal dosing in acute pancreatitis pai management (5,8-10,16-20).
Limitations
This report has several limitations. First, the sample size was extremely small, with only two patients included, which limits the scope and generalizability of the findings. Second, the observational nature of the report, together with the absence of a control group does not allow definitive conclusions regarding the efficacy of low-dose ketamine to be established. In addition, analgesic outcomes were assessed only in the short term, without evaluation of prolonged effects or pain recurrence. Finally, follow-up duration was not standardized
between the two cases.
Conclusions
Low-dose intravenous ketamine provided rapid and effective analgesia in two cases of severe acute pancreatitis refractory to conventional treatment. These findings suggest that ketamine may be considered as a rescue analgesic option in selected patients, particulary in opioid-resistant pain states. Further prospective controlled studies are required to determine optimal dosing, safety, and long-terme outcomes.
References
- Meng W, Yuan J, Zhang C, Bai Z, Zhou W, Yan J, et al. Parenteral analgesics for pain relief in acute pancreatitis : a systematic review. Pancreatology. 2013:13(3):201(206.
- Wu Y, Han C, Luo R, Cai W, Xia Q, Jiang R, et al. Molecular mechanisms of pain in acute pancreatitis: recent basic research advances and therapeutic implications. Front Neurosci. 2023;16:13331438.
- Bouwense SAW, Buscher HCJL, Van Goor H, Wilder-Smith OHG. S-ketamine modulates hyperalgesia in patients with chronic pancreatitis pain. Reg Anesth Pain Med. 2011;36(3):303- 307.
- Zerem E.Treatment of severe acute pancreatitis and its complications.World J Gastroenterol. 2014;20(38):13879–13891.PMID: 25320523.
- Orhurhu VJ, Roberts JS, Ly NK, Cohen SP. Ketamine in acute and chronic pain management. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023.
- Doan LV, Wang J. An update on the basic and clinical science of ketamine analgesia. Clin J Pain. 2018;34(11):1077-1088.
- Duong HG, Pulskamp TG, Berlau DJ. Ketamine for acute and chronic pain: beyond anaesthesia. Pain Manag. May 2026;16(5) : 523-533.
- Zhou JS, Peng GF, Liang WD, Chen Z, Liu YY, Wang BY, et al. Recent advances in the study of anesthesia- and analgesia-related mechanisms of S-ketamine. Front Pharmacol. 2023;14:1228895.
- Schwenk ES, Viscusi ER, Buvanendran A, Hurley RW, Wasan AD, Narouze S, et al. Consensus guidelines on the use of intravenous ketamine infusions for acute pain management. Reg Anesth Pain Med. 2018;43(5):456-466.
- Motov S, Mai M, Pushkar I, Likourezos A, Drapkin J, Yasavolian M, et al. A prospective randomized, double-dummy trial comparing IV push low-dose ketamine to short infusion of low-dose ketamine for treatment of pain in the ED. Am J Emerg Med. 2017;35(8):1095-1100.
- Fasanella KE, Davis B, Lyons J, Chen ZM, Lee KK. Ketamine use for successful resolution of post-ERCP acute pancreatitis abdominal pain. Case Rep Anesthesiol. 2017;2017:7845368.
- Yaksh TL, Woller SA, Ramachandran R, Sorkin LS. The search for novel analgesics: targets and mechanisms. F1000Prime Rep. May 2015;7:56.
- Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain. Pain. 2011;152(3 Suppl):S2-S15.
- Rael Frances Bell. Eija Anneli Kalso. Ketamine for pain management. Pain Rep. 2018. Aug 9;3(5):e674.
- Niesters M, Martini C, Dahan A. Ketamine for chronic pain: risks and benefits. Br J Clin Pharmacol. 2014;77(2):357-367.
- Green SM, Roback MG, Krauss B, Miner JR, Schneider S, Kivela PD, et al. Unscheduled procedural sedation: a multidisciplinary consensus practice guideline. Ann Emerg Med. 2019;73(5):e51-e65.
- Cohen SP, Bhatia A, Buvanendran A, Schwenk ES, Wasan AD, Hurley RW, et al. Consensus guidelines on intravenous ketamine infusions for chronic pain. Reg Anesth Pain Med. 2018;43(5):521-546.
- Visser E, Schug SA. The role of ketamine in pain management. Biomed Pharmacother. 2006;60(7):341-348.
- Persson J. Ketamine in pain management. CNS Neurosci Ther. 2013;19(6):396-402.
- Loftus RW, Yeager MP, Clark JA, Brown JR, Abdu WA, Sengupta DK, et al. Intraoperative ketamine reduces perioperative opioid analgesic requirements. Anesthesiology. 2010;113(3):639-646.