
Abstract
Background: Intrathecal (IT) opioid trialing is a recommended practice before implantation of a permanent intrathecal drug delivery system. Most described techniques, however, do not allow flexible dose titration to balance analgesic efficacy with adverse reactions. Objective: To describe the clinical experience with an IT opioid trialing protocol combining patient-controlled analgesia (PCA) bolus doses and continuous infusion, using a self-evaluation chart to assess analgesia, adverse events, and patient satisfaction in 13 chronic non-cancer pain patients. Methods: Thirteen patients (mean age 70 years, range 36–90) refractory to oral/transdermal (TD) strong opioids underwent a 4-day inpatient IT trial using a portable PCA pump. An initial IT morphine bolus (0.10–0.30 mg) was followed by stepwise PCA titration, addition of a continuous basal infusion on Day 2, conversion to full continuous infusion on Day 3, and formal satisfaction evaluation on Day 4. A structured self-evaluation chart documented pain (VAS) and adverse events throughout. Results: All patients were evaluated for analgesia and adverse events. Dose adjustments were made based on efficacy/safety profiles. Two patients required urinary catheterization; one could not achieve an analgesic dose. One patient discontinued due to intolerable urinary incontinence. Most patients who completed the protocol expressed satisfaction. Conclusions: This standardized protocol combining PCA and continuous infusion enables individualized IT morphine titration with an acceptable safety profile. Patient-driven self-evaluation facilitates the analgesia–adverse event balance. The portable PCA pump provides a realistic preview of implantable pump therapy. Validation in a larger cohort is warranted.
Introduction
Intrathecal (IT) drug delivery is an established treatment modality for patients with refractory chronic non-cancer pain who have not responded adequately to conventional pharmacological therapies [1,2]. Prior to implanting a permanent intrathecal pump, a trialing phase is widely recommended to confirm analgesic efficacy and identify potential adverse reactions at the individual level [1–6].
The Polyanalgesic Consensus Conference (PACC® 2024) concludes that no single trialing method has demonstrated superiority over others in non-cancer pain, with comparable levels of evidence supporting single-shot, bolus, and continuous infusion approaches [1]. A critical limitation of most currently described trialing techniques is the absence of a flexible titration strategy, which is essential to achieve an individualized balance between analgesia and adverse effects [1,2,3,8,9]. Furthermore, trial duration is relevant: prolonged trials may increase the risk of catheter-related complications.
We previously presented a novel IT opioid trialing protocol at the IASP 2024 World Congress on Pain (Abstract TH667, Amsterdam, Netherlands), combining continuous infusion with PCA rescue bolus doses via a portable external pump. This approach allows stepwise dose titration and an infusion profile that resembles that of an implanted pump. In this report, we present the clinical experience with this protocol — termed PAIN-PRE (Protocolo de Analgesia INtratecal PRE-Implante) — in 13 patients with chronic non-cancer pain, incorporating a structured self-evaluation chart.
The Polyanalgesic Consensus Conference (PACC® 2024) concludes that no single trialing method has demonstrated superiority over others in non-cancer pain, with comparable levels of evidence supporting single-shot, bolus, and continuous infusion approaches [1]. A critical limitation of most currently described trialing techniques is the absence of a flexible titration strategy, which is essential to achieve an individualized balance between analgesia and adverse effects [1,2,3,8,9]. Furthermore, trial duration is relevant: prolonged trials may increase the risk of catheter-related complications.
We previously presented a novel IT opioid trialing protocol at the IASP 2024 World Congress on Pain (Abstract TH667, Amsterdam, Netherlands), combining continuous infusion with PCA rescue bolus doses via a portable external pump. This approach allows stepwise dose titration and an infusion profile that resembles that of an implanted pump. In this report, we present the clinical experience with this protocol — termed PAIN-PRE (Protocolo de Analgesia INtratecal PRE-Implante) — in 13 patients with chronic non-cancer pain, incorporating a structured self-evaluation chart.
Materials & Methods
Patient Selection
Thirteen consecutive patients with chronic non-cancer pain were enrolled from January 2016 to September 2025 at Fundación CENIT, Buenos Aires, Argentina. Inclusion criteria were: (1) chronic non-cancer pain refractory to optimized oral or TD strong opioid therapy; (2) completion of clinical and psychological evaluation by the treating team; and (3) agreement to undergo an inpatient IT opioid trial with potential for permanent pump implantation.
IT Trialing Protocol
A tunneled intrathecal catheter was placed under fluoroscopic guidance and connected to a portable PCA external pump (Figure 1). The initial IT morphine bolus dose was individualized according to the total daily oral/TD opioid dose, ranging from 0.10 to 0.30 mg.
Day 1: After the initial bolus, patients were evaluated at 30 and 60 minutes for adverse effects. A structured self-evaluation chart (Figure 2) was completed, documenting pain intensity and adverse events — itching, nausea, vomiting, shortness of breath, and urinary retention — on a Visual Analogue Scale (VAS, 0–10). PCA bolus settings were programmed based on the first-dose efficacy/safety profile, with a 10-hour lockout for the first 24 hours. Patients completed the chart before and after each PCA bolus.
Day 2: Analgesia and adverse events were re-assessed. Based on the 24-hour IT morphine requirement, PCA bolus doses were adjusted or a continuous basal infusion was initiated at 50% of the total 24-hour morphine dose. PCA rescue bolus doses were set at 10–15% of the daily dose with a 4-hour lockout period.
Day 3: If analgesia and adverse event profiles were well balanced, the 24-hour morphine requirement was converted to full continuous infusion, mimicking the functioning of a permanent implantable pump under real-life conditions.
Day 4: If analgesia and adverse events remained balanced, patients rated the procedure using a 5-point satisfaction scale: Very Satisfied (VS), Moderately Satisfied (MS), Poorly Satisfied (PS), Unsatisfied (U), or Not Able to Evaluate (NR). The evaluation chart was signed by both patient and physician in the presence of a witness, constituting a formal agreement to proceed with permanent pump implantation if the patient was satisfied.
Outcome Measures
Primary outcomes included: (1) change in pain VAS from pre-trial baseline to Day 4; (2) final daily IT morphine dose; (3) adverse events during the trial; and (4) patient satisfaction rating at Day 4.
Thirteen consecutive patients with chronic non-cancer pain were enrolled from January 2016 to September 2025 at Fundación CENIT, Buenos Aires, Argentina. Inclusion criteria were: (1) chronic non-cancer pain refractory to optimized oral or TD strong opioid therapy; (2) completion of clinical and psychological evaluation by the treating team; and (3) agreement to undergo an inpatient IT opioid trial with potential for permanent pump implantation.
IT Trialing Protocol
A tunneled intrathecal catheter was placed under fluoroscopic guidance and connected to a portable PCA external pump (Figure 1). The initial IT morphine bolus dose was individualized according to the total daily oral/TD opioid dose, ranging from 0.10 to 0.30 mg.
Day 1: After the initial bolus, patients were evaluated at 30 and 60 minutes for adverse effects. A structured self-evaluation chart (Figure 2) was completed, documenting pain intensity and adverse events — itching, nausea, vomiting, shortness of breath, and urinary retention — on a Visual Analogue Scale (VAS, 0–10). PCA bolus settings were programmed based on the first-dose efficacy/safety profile, with a 10-hour lockout for the first 24 hours. Patients completed the chart before and after each PCA bolus.
Day 2: Analgesia and adverse events were re-assessed. Based on the 24-hour IT morphine requirement, PCA bolus doses were adjusted or a continuous basal infusion was initiated at 50% of the total 24-hour morphine dose. PCA rescue bolus doses were set at 10–15% of the daily dose with a 4-hour lockout period.
Day 3: If analgesia and adverse event profiles were well balanced, the 24-hour morphine requirement was converted to full continuous infusion, mimicking the functioning of a permanent implantable pump under real-life conditions.
Day 4: If analgesia and adverse events remained balanced, patients rated the procedure using a 5-point satisfaction scale: Very Satisfied (VS), Moderately Satisfied (MS), Poorly Satisfied (PS), Unsatisfied (U), or Not Able to Evaluate (NR). The evaluation chart was signed by both patient and physician in the presence of a witness, constituting a formal agreement to proceed with permanent pump implantation if the patient was satisfied.
Outcome Measures
Primary outcomes included: (1) change in pain VAS from pre-trial baseline to Day 4; (2) final daily IT morphine dose; (3) adverse events during the trial; and (4) patient satisfaction rating at Day 4.
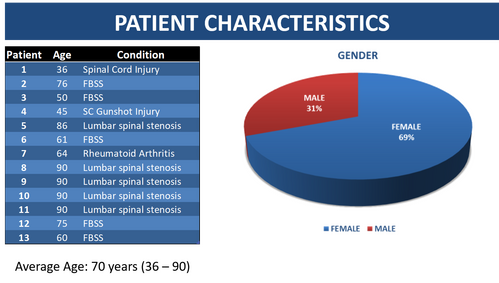
Figure 3. Patient Characteristics
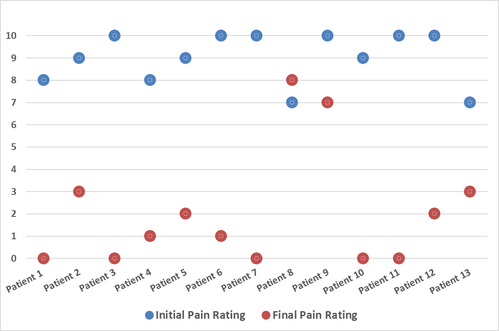
Figure 5. INITIAL – FINAL ANALGESIA (VAS)
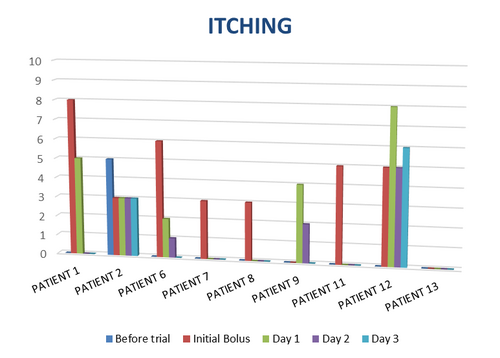
Figure 7. ITCHING
Results
Patient Characteristics
Thirteen patients were included (mean age 70 years, range 36–90). All were receiving oral or TD strong opioids with inadequate pain control prior to enrollment. Patients presented with various chronic non-cancer pain conditions (figure 3).
IT Morphine Doses and Analgesic Outcomes
Initial IT morphine doses ranged from 0.10 to 0.30 mg, individualized per patient. The protocol allowed stepwise titration across the 4-day trial in all evaluable patients. Initial and final daily IT morphine doses are presented in Figure 4. Initial and final VAS pain scores are shown in figure 5. All evaluable patients demonstrated measurable reduction in pain VAS from baseline to trial completion.
Adverse Events
Adverse events were monitored prospectively via the self-evaluation chart and managed primarily through IT morphine dose adjustment (Figure 6). Two patients developed urinary retention requiring catheterization; in both, the complication resolved with dose reduction. One of these patients was unable to reach an effective analgesic dose within the trial period. One patient with a prior history of urinary incontinence surgery experienced intolerable urinary incontinence during the trial, necessitating early discontinuation [10]. 6 patients developed itching after the first bolus dose or dose increase, resolving after dose adjustment in 5 of them while only one did not tolerate it and decided not to be implanted (figure 7). No serious adverse events such as respiratory depression or refractory nausea/vomiting were recorded.
Patient Satisfaction
Patient satisfaction at Day 4 is summarized in Figure 8. 10 patients who completed the full 4-day protocol expressed satisfaction with the procedure, and signed the evaluation chart agreeing to proceed with permanent pump implantation. 3 patients rated the trial as poorly satisfied/unsatisfied because of urinary dysfunction or intolerable itching and did not agree to be implanted.
Discussion
The PAIN-PRE protocol offers several practical advantages over conventional IT trialing methods. First, the structured PCA titration phase provides the flexibility needed to individualize morphine dosing to each patient's analgesic requirements and adverse event profile. Second, the transition to full continuous infusion on Day 3 closely resembles the functioning of a permanent implantable pump, offering both patients and clinicians a realistic preview of long-term therapy before a surgical implant decision is made. Third, the use of the self-evaluation chart throughout the trial actively engages patients in their own care, systematically documenting pain scores and adverse events to guide daily dose adjustments. This patient-centered approach aligns with current best practice guidelines that emphasize shared decision-making in interventional pain management [1,5,6].
The low IT morphine doses required in this protocol are consistent with PACC recommendations for non-cancer pain and minimize the risk of adverse events associated with higher doses [1,7]. The 4-day structured timeline balances the need for adequate titration and assessment with the goal of limiting catheter-related complications from prolonged trials.
Thirteen patients were included (mean age 70 years, range 36–90). All were receiving oral or TD strong opioids with inadequate pain control prior to enrollment. Patients presented with various chronic non-cancer pain conditions (figure 3).
IT Morphine Doses and Analgesic Outcomes
Initial IT morphine doses ranged from 0.10 to 0.30 mg, individualized per patient. The protocol allowed stepwise titration across the 4-day trial in all evaluable patients. Initial and final daily IT morphine doses are presented in Figure 4. Initial and final VAS pain scores are shown in figure 5. All evaluable patients demonstrated measurable reduction in pain VAS from baseline to trial completion.
Adverse Events
Adverse events were monitored prospectively via the self-evaluation chart and managed primarily through IT morphine dose adjustment (Figure 6). Two patients developed urinary retention requiring catheterization; in both, the complication resolved with dose reduction. One of these patients was unable to reach an effective analgesic dose within the trial period. One patient with a prior history of urinary incontinence surgery experienced intolerable urinary incontinence during the trial, necessitating early discontinuation [10]. 6 patients developed itching after the first bolus dose or dose increase, resolving after dose adjustment in 5 of them while only one did not tolerate it and decided not to be implanted (figure 7). No serious adverse events such as respiratory depression or refractory nausea/vomiting were recorded.
Patient Satisfaction
Patient satisfaction at Day 4 is summarized in Figure 8. 10 patients who completed the full 4-day protocol expressed satisfaction with the procedure, and signed the evaluation chart agreeing to proceed with permanent pump implantation. 3 patients rated the trial as poorly satisfied/unsatisfied because of urinary dysfunction or intolerable itching and did not agree to be implanted.
Discussion
The PAIN-PRE protocol offers several practical advantages over conventional IT trialing methods. First, the structured PCA titration phase provides the flexibility needed to individualize morphine dosing to each patient's analgesic requirements and adverse event profile. Second, the transition to full continuous infusion on Day 3 closely resembles the functioning of a permanent implantable pump, offering both patients and clinicians a realistic preview of long-term therapy before a surgical implant decision is made. Third, the use of the self-evaluation chart throughout the trial actively engages patients in their own care, systematically documenting pain scores and adverse events to guide daily dose adjustments. This patient-centered approach aligns with current best practice guidelines that emphasize shared decision-making in interventional pain management [1,5,6].
The low IT morphine doses required in this protocol are consistent with PACC recommendations for non-cancer pain and minimize the risk of adverse events associated with higher doses [1,7]. The 4-day structured timeline balances the need for adequate titration and assessment with the goal of limiting catheter-related complications from prolonged trials.
Conclusions
A standardized IT opioid trialing protocol combining PCA bolus and continuous infusion with a structured self-evaluation chart is feasible, well-tolerated, and informative in patients with chronic non-cancer pain. The protocol allows individualized dose titration with an acceptable safety profile, actively involves patients in outcome monitoring, and provides a realistic simulation of permanent pump therapy. The limited sample size of 13 patients warrants validation in a larger, prospective cohort to confirm the utility and generalizability of this approach.
Figures

Figure 1. Tunnelled catheter and PCA pump (bandages were taken off for visual purposes).
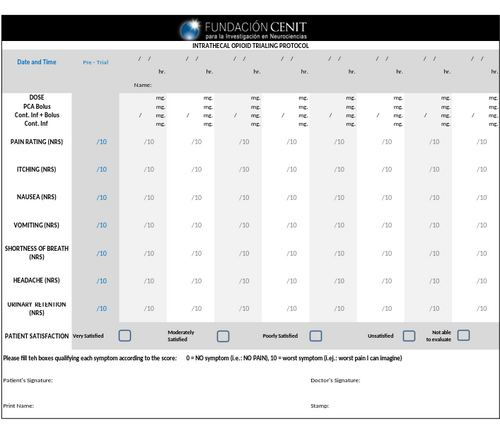
Figure 2. Chart to document pain & AE ratings pre-trial, during trial and patient satisfaction. Pump parameters and daily morphine requirements are documented.
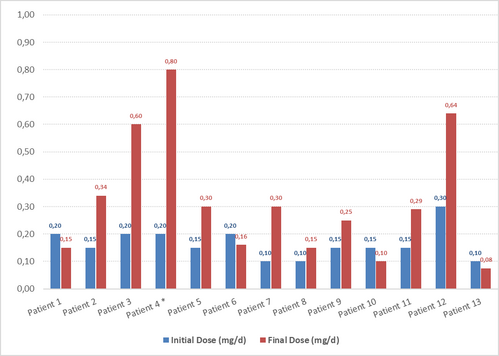
Figure 4. IT MORPHINE DOSE
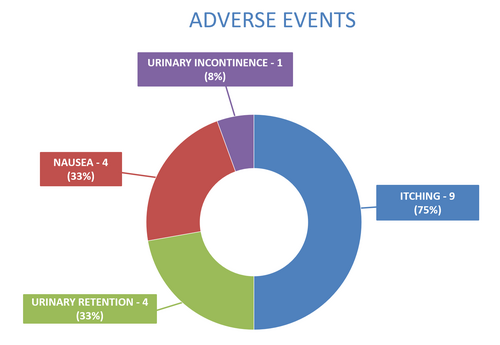
Figure 6. ADVERSE EVENTS
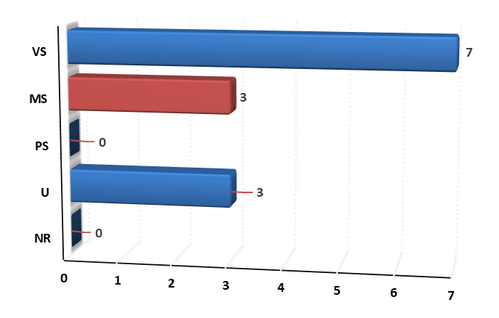
Figure 8. PATIENT SATISFACTION ( VS: Very Satisfied, MS: Moderately Satisfied, PS: Poorly Satisfied, U: Unsatisfied, NR: Not able to evaluate)
References
- Deer TR, Hayek SM, et al. The Polyanalgesic Consensus Conference (PACC)®: Intrathecal Drug Delivery Guidance on Safety and Therapy Optimization When Treating Chronic Noncancer Pain. Neuromodulation. 2024 Oct;27(7):1107-1139.
- Bolash R, Mekhail N. Intrathecal pain pumps: indications, patient selection, techniques, and outcomes. Neurosurg Clin N Am. 2014 Oct;25(4):735-42
- Prager J, Deer T et al. Best practices for intrathecal drug delivery for pain. Neuromodulation. 2014 Jun; 17(4):354-72.,
- Raffaeli W, et al. Intraspinal therapy for the treatment of chronic pain: a review of the literature between 1990 and 2005 and suggested protocol for its rational and safe use. Neuromodulation. 2006 Oct;9(4):290-308
- Pope, J, Deer, T et al. Clinical Uses of Intrathecal Therapy and Its Placement in the Pain Care Algorithm. Article first published online: 23 FEB 2016
- Deer T, Chapple I, et al. Intrathecal drug delivery for treatment of chronic low back pain: report from the National Outcomes Registry for Low Back Pain. Pain Med. 2004 Mar; 5(1):6-13.
- Bottros MM, Christo PJ. Current perspectives on intrathecal drug delivery. J Pain Res. 2014 Nov 6;7:615-26
- Grider JS, Harned ME, Etscheidt MA. Patient selection and outcomes using a low-dose intrathecal opioid trialing method for chronic nonmalignant pain. Pain Physician. 2011 Jul-Aug; 14(4):343-51.
- Ruan X, Couch JP. Unique low-dose intrathecal opioid trial, still in need of a feasibility check. Pain Physician. 2011 Sep-Oct;14(5):E462-3
- Kuipers PW1, Kamphuis ET, van Venrooij GE, van Roy JP, Ionescu TI, Knape JT, Kalkman CJ. Intrathecal opioids and lower urinary tract function: a urodynamic evaluation. Anesthesiology. 2004 Jun;100(6):1497-503.
Conflicts of Interest
The authors declare no conflicts of interest.
Funding Statement
This research did not receive specific external funding and was performed as part of the regular clinical activity of the authors at Fundación CENIT, Buenos Aires, Argentina.