
Audio Presentation
Abstract
Andersson lesions (AL) are rare destructive discovertebral lesions found in patients with ankylosing spondylitis (AS), characterized by areas of bone destruction and sclerosis at the vertebral endplates and intervertebral discs. ALs can be found in 85.5% of AS patients via whole-spine MRI, but only identified at 37.5% with plain radiographs, suggesting an
underestimated true prevalence of these lesions [1]. ALs cause chronic pain, resulting in significant reductions in quality of life. Management for ALs ranges from conservative measures, including physiotherapy and pharmacological interventions, to surgical solutions such as spinal instrumentation and fusion [2]. There is a notable gap in the literature addressing alternative therapeutic options for patients with symptomatic ALs who fail conservative treatment but are not candidates for surgery.
underestimated true prevalence of these lesions [1]. ALs cause chronic pain, resulting in significant reductions in quality of life. Management for ALs ranges from conservative measures, including physiotherapy and pharmacological interventions, to surgical solutions such as spinal instrumentation and fusion [2]. There is a notable gap in the literature addressing alternative therapeutic options for patients with symptomatic ALs who fail conservative treatment but are not candidates for surgery.
Introduction
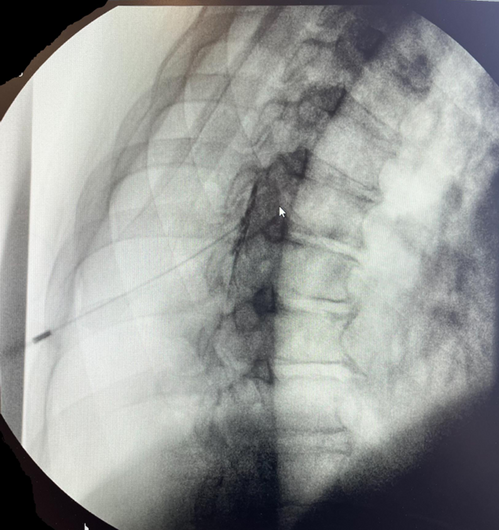
Our patient is a 59 year-old male with longstanding AS and worsening ten-year history of mid- thoracic, lumbar, and sacral pain. Prior medical treatments included physiotherapy and opioids with minimal relief. Sacral pain improved with sacroiliac joint injections and medial branch blocks. AS was managed w/ methotrexate, etanercept, and leflunomide. Initial bone scan showed increased signaling at antero-superior corner of T8 body, with repeat scans showing T8-9 edema, possibly a spinal hemangioma. Due to complicated atypical tuberculosis cellulitis, biologics were discontinued, resulting in thoracic pain refractory to strong opioid use. Repeat CT showed luceny/erosion at inferior endplate of T7. US Guided T7-T8 erector spinae block provided moderate relief while biologics were held during antibiotic therapy. After adalimumab was resumed, left paramedial T6-T7 epidural steroid injection provided 90% relief. In follow up MRI, resolution of T7 edema was noted with chronic Schmorl’s node formation, indicating lesion was likely an undiagnosed AL.
Materials & Methods
Non applicable

Results
AS complicated by ALs is an under-diagnosed condition that can significantly impact patients’ quality of life. Currently researched treatment options overlook other interventions for pain relief beyond pharmacotherapy, conservative treatment, and surgical intervention. We present a case where ESP and ESI provided greater than 1 year of 60-90% relief for a patient with a history of ineffective conservative and pharmacologic treatment that was not an appropriate surgical candidate. This successful intervention offers a potential treatment options for clinicians managing thoracic pain caused by AS complicated by ALs, underscores the need for further awareness and research of AL management.
Conclusions
In patients with AS complicated by ALs, timely diagnosis and appropriate management are crucial to improving outcomes and quality of life. This case highlights the potential role of epidural steroid injections as a bridge for acute pain relief when conservative measures fail, and surgical interventions are not feasible. Further research is needed to validate the efficacy
of ESIs and refine pain management guidelines for this challenging condition.
of ESIs and refine pain management guidelines for this challenging condition.
Figures

References
[1] Huang JC, Qian BP, Qiu Y, Wang B, Yu Y, Zhao SZ. Occult Andersson lesions in patients with ankylosing spondylitis: undetectable destructive lesions on plain radiographs. Chin Med J (Engl). 2021 Jun 4;134(12):1441-1449. doi: 10.1097/CM9.0000000000001557. PMID: 34091520; PMCID: PMC8213248.
[2] Bittar M, Deodhar A. Axial Spondyloarthritis: A Review. JAMA. 2024 Dec 4. doi: 10.1001/jama.2024.20917.Epub ahead of print. PMID: 39630439.
[2] Bittar M, Deodhar A. Axial Spondyloarthritis: A Review. JAMA. 2024 Dec 4. doi: 10.1001/jama.2024.20917.Epub ahead of print. PMID: 39630439.
Conflicts of Interest
There are no conflicts of interests for this case report.
Funding Statement
Non applicable.